
Healing at the Speed of Light: The Use of Light Therapy for Tendon Healing (June '25)
Jun 10, 2025At the Tendon and Joint Healing Academy, our mission is to empower highly motivated, active individuals with knowledge on their journey to healing and recovery from musculoskeletal injuries.
Learning Objectives:
Understand the use of light and specific light frequencies for tendon healing
To do this we must:
- Understand the importance of circadian rhythms in healing
- Understand what photobiomodulation (PBM) therapy is and how it works
- Understand the role of PBM therapy on pain, inflammation, tissue healing, and cellular energy production
- Focus on studies in the medical literature using PBM for tendon healing especially for chronic tendinopathy
Give me the Easy Version…
Imagine harnessing the power of light to help your body heal. It might sound like science fiction, but it's real! In this article, we'll explore how different types of light can be used to treat tendon injuries and promote overall health.
Your body's internal clock, known as your circadian rhythm, plays a crucial role in healing. To keep it in sync, spend time in natural light during the day and ensure complete darkness at night. This helps set the stage for even greater improvements when using light therapy.
What is photobiomodulation therapy?
Photobiomodulation therapy (PBM), also called low-level light therapy, is like a supercharged flashlight for your cells. It uses specific wavelengths of light to repair tissues, reduce inflammation, and ease pain. Don't worry; it doesn't involve lasers that burn or cut. The wavelengths of light are typically in the red and near-infrared range.
How PBM Works:
Your body's cells contain tiny power plants called mitochondria. PBM excites these power plants with light, especially in the red and near-infrared range. This energy boost helps create more fuel (ATP) and even reduces inflammation and promotes tissue healing.
Pain Relief in Minutes:
PBM doesn't take long to work. Within minutes, it can block pain signals, relax muscles, and reduce muscle spasms. So, if you're suffering, relief is just a few minutes away.
Long-Term Benefits:
The effects of PBM can last for months or even years. Over time, it can promote tissue healing, reduce inflammation, and improve overall function.
Tackling Tendon Troubles: Now, let's focus on how PBM can specifically help with tendon problems. Studies show that it can boost collagen production and reduce inflammation in tendons, which are critical for healing.
Combining PBM with Exercise:
Exercise is excellent for tendon health, but what if PBM could make it even better? In some cases, PBM combined with exercise (such as with Achilles tendinitis) has shown remarkable results. It reduces pain, improves function, and could even mean less exercise overall.
Promising Results:
While more research is needed, PBM holds great promise for treating tendon injuries. It's safe without any real side effects reported in the literature and is non-invasive, meaning no needles or painful procedures. Remember, light therapy is just one piece of the puzzle. For the best results, combine it with education, exercise, lifestyle changes, and activity modifications. By embracing this holistic approach, you can shine a light on your path to healing.
Give me the Details…
Imagine harnessing the power of light to help your body heal. It might sound like science fiction, but it's real! In this article, we'll explore how different types of light can be used to treat tendon injuries and promote overall well-being.
The most foundational step on the way to using light to assist with tendon healing is through entrainment of your circadian rhythm from appropriate light exposure. This means getting outside and seeing the sun, especially in the morning and having a period of complete darkness at night. (If you have not yet read this article, start here- Don’t be Late: The Importance of Timing in Musculoskeletal Health).
However, specific wavelengths of light can be used to treat specific musculoskeletal conditions. It is even proposed that light is a drug equivalent, which is a powerful statement 1.
Photobiomodulation (PBM) also known as low-level light therapy (LLLT) is the application of light with the purpose of promoting tissue repair, decreasing inflammation, and reducing pain. This is usually done by way of a low-power light source such as LED (light-emitting diode) or a LASER (Light Amplification by Stimulated Emission of Radiation). The treatment causes no significant temperature rise or gross tissue structure change in the tissue being targeted for treatment 2. Light wavelengths between 600 to 700nm and 780 to 1100 nm, which is the red to near infrared spectrum, are typically used because these wavelengths can penetrate skin, and soft/hard tissues. The issue is that studies sometimes do not use the same frequency or dose of light to treat the same condition. In general, at low doses (up to 2 J cm−2), PBM stimulates proliferation, whereas at higher doses (16 J cm−2 or higher) PBM is suppressive 2. In general, a biphasic dose response has been observed where low levels of light improve tissue repair compared to high levels. Biological processes are stimulated at relatively low levels of energy density, and the positive effect diminishes as the dose increases and inhibitory effects eventually predominate. A systematic review on PBM therapy for treatment of tendinopathy found that 11 out of 20 studies failed to produce a positive result. However, the likely reason for failure was either the laser power density was too high, or the treatment time was too long 3.
Photobiomodulation has been studied in numerous orthopedic conditions including ligamentous sprains, muscular strains, osteoarthritis, neck and back pain, and tendinopathy just to name a few 4.
How does it work?
First, energy carrying photons from a light source need to be absorbed by electrons belonging to a photoreceptor or chromophore of the targeted tissue. A chromophore is a molecule (or portion of a molecule) which imparts a color to a compound. Some examples of chromophores include chlorophyll, hemoglobin, myoglobin, cytochrome c oxidase). A significant target of light in humans are mitochondria, the so called “power plants” of our cells which turn electrons from food into energy (ATP) and also make water 4. Excitation of the 4th mitochondrial complex, cytochrome c oxidase (CCO), serves as the primary photon acceptor in the red and near infrared region and serves an essential target site in photobiomodulation. Cytochrome c oxidase is the last complex in the mitochondrial electron transport chain and is composed of 2 heme centers and 2 copper centers. When light hits CCO, photon energy is absorbed by the metal centers which excites electrons from their ground states. Light also causes dissociation of nitric oxide from CCO (see image below)5.
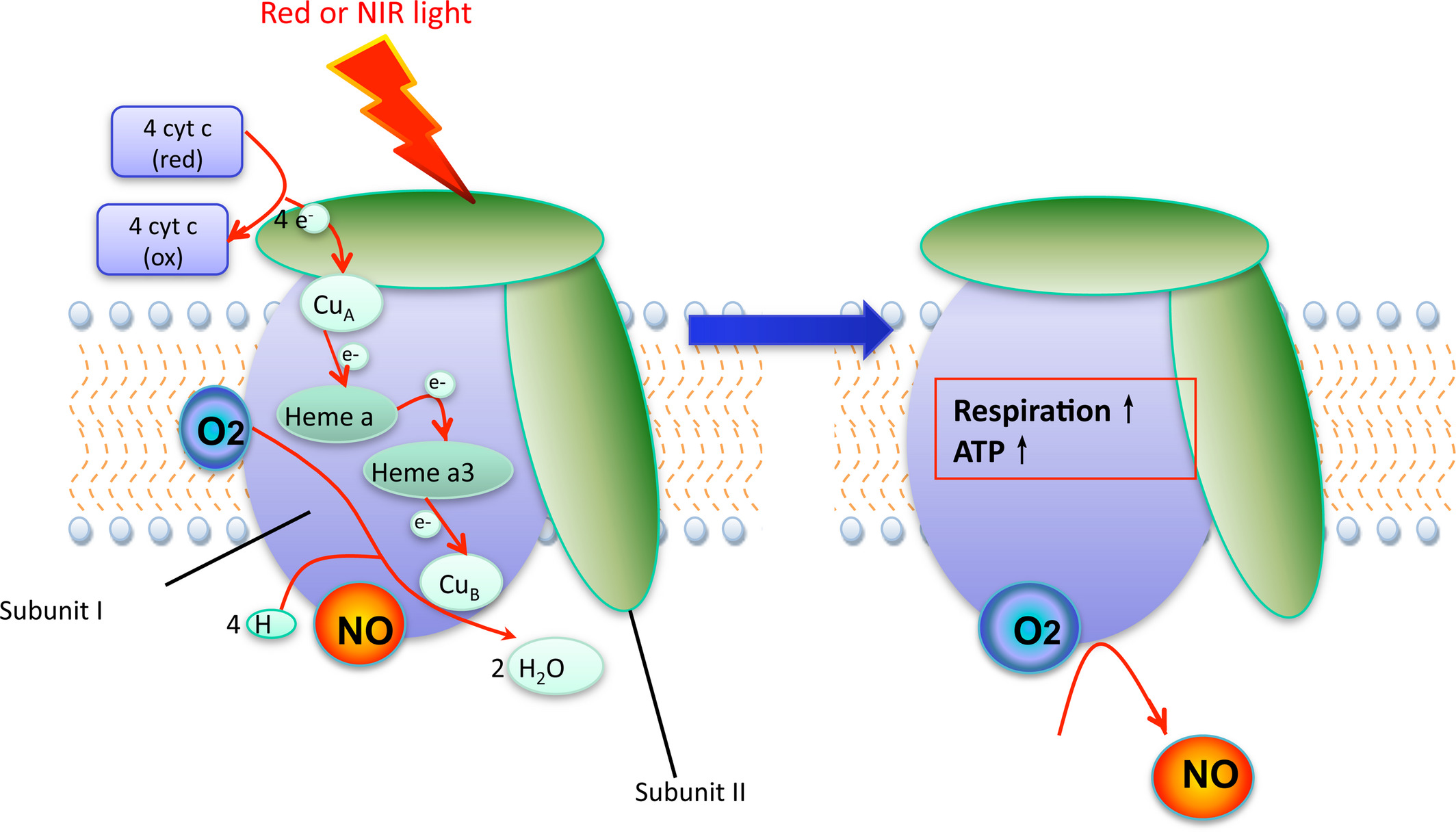
Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochem Photobiol. 2018;94(2):199-212
Since nitric oxide inhibits electron transport in the mitochondria, dissociation of NO can increase the mitochondrial membrane potential, increase oxygen consumption, and therefore increase the proton gradient which leads to an increase in ATP production. Next comes the production of reactive oxygen species, release of calcium as a second messenger leading to activation of transcription factors and signaling mediators to result in long lasting effects on cells. This is depicted below with light eventually leading to gene transcription 4.
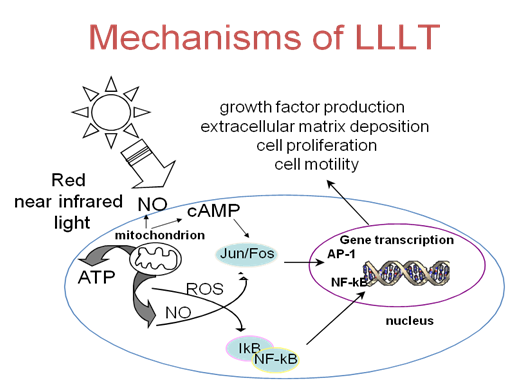
Cotler HB, Chow RT, Hamblin MR, Carroll J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop Rheumatol. 2015;2(5).
So, is the above paragraph saying that you can stimulate energy production and downstream cellular effects such as tissue healing and reduced inflammation without the use of food, pills, or exercise?
YES, IT IS. This is all possible by the actions of light.
Photobiomodulation can also lead to pain relief. Fast acting pain relief occurs within minutes of application as the result of neural blockade of the peripheral and sympathetic nerves and release of neuromuscular contractions leading to reduced muscle spasm. Within hours to days there is a decrease in local edema and inflammation. Long term effects occur within 1-2 weeks and can last for months and sometime years due to improved tissue healing. There are multiple clinical targets for PBM including 1. the actual site of injury to promote tissue healing, remodeling, and reducing inflammation, 2. Lymph nodes to reduce edema and inflammation, 3. Nerves to cause analgesia, and 4. Trigger points to reduce muscle spasm 4.
Now that we have a basic understanding of photobiomodulation, let’s take a deeper look into the evidence specifically for tendons.
In vitro studies and animal studies have shown that PBM can increase the expression of genes related to type I collagen and decrease the expression of genes related to inflammation such as TNF-α and IL-6 in tenocytes. In human studies, PBM combined with exercise has shown significant reduction in pain levels and improved function compared to sham treatment plus exercise. Also, when compared to other interventions such as anti-inflammatory medications, corticosteroid injections, and iontophoresis, PBM was equally effective as reducing pain. This alone is great as PBM is non-invasive and much safer than medications and injections. However, this review noted that the studies were of low to moderate quality evidence 6.
We have previously discussed the great importance of using exercise by way of the concept of mechanotransduction to help heal a tendon. This is certainly the basis of treatment of tendinopathy. However, what if light by way of PBM treatment can help to augment the effect of exercise? Also, if we look at Achilles tendinopathy, the typical Alfredson eccentric protocol required 3 sets of 15 repetitions twice daily both with the knee straight and with the knee bent done over a period of 12 weeks.
One study looked to see if similar results could be obtained by only 2 sessions per week and if the addition of PBM therapy would bring added benefit. The study included 80 individuals with chronic achilles tendinopathy > 3 months. The laser protocol used 810 and 980 nm light. Total energy delivered was 450 J at an energy density of 6.66 J/cm2 and was completed prior to exercise sessions during the first 4 weeks only. The exercise protocol included heavy load eccentric exercise either twice per day every day or once per day and only twice per week for 12 weeks (also leaving 2-3 days in between exercise). There were 4 groups: group 1- Placebo + daily exercise, group 2- laser + daily exercise, group 3- placebo + exercise twice per week, group 4 laser + exercise twice per week. The maximum number of exercise sessions in the regular exercise group was a whopping 168, compared to a measly 24 in the reduced exercise group. Keep these numbers in mind.
Using the VISA-A score, group 4 (laser + reduced exercise) had significant functional improvement at 12 weeks compared to the other groups. There was a moderate effect size for the reduced exercise regimen over the typical daily exercise protocol. Let me reiterate those findings again. Although not statistically significant, the reduced exercise group did slightly better than the twice daily exercise group. The addition of PBM laser treatment also offered additional gains in the twice per week exercise protocol group only at 12 weeks. The authors discuss how the reduced exercise protocol group were likely able to take full effect of mechanotransduction after their exercise sessions as loading a tendon stimulates remodeling with a peak effect 72 hours post exercise. The reduced exercise group was instructed to leave 2–3 days between exercise sessions in order to gain the full benefit of mechanotransduction. The other benefit of the reduced exercise protocol was a fantastic compliance rate at 100% compared to only 70% of those in the daily exercise group 7.
Photobiomodulation therapy has great promise in the treatment of tendinopathy given its potential to enhance the tendon tissue repair and remodeling process required for the eventual resolution of tendinopathy. It is also favorable given that it is non-invasive, pain free, and requires little application time. And remember, as with any specific intervention, photobiomodulation should be used in a comprehensive approach combined with education, exercise, lifestyle, and activity modifications. Most importantly, the best photobiomodulation is using the sun. The sun is also free! Go outside and exercise!
- Karu T. Is it time to consider photobiomodulation as a drug equivalent? Photomed Laser Surg. 2013;31(5):189-191.
- de Freitas LF, Hamblin MR. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J Sel Top Quantum Electron. 2016;22(3).
- Tumilty S, Munn J, McDonough S, Hurley DA, Basford JR, Baxter GD. Low level laser treatment of tendinopathy: a systematic review with meta-analysis. Photomed Laser Surg. 2010;28(1):3-16.
- Cotler HB, Chow RT, Hamblin MR, Carroll J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop Rheumatol. 2015;2(5).
- Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochem Photobiol. 2018;94(2):199-212.
- Tripodi N, Feehan J, Husaric M, Sidiroglou F, Apostolopoulos V. The effect of low-level red and near-infrared photobiomodulation on pain and function in tendinopathy: a systematic review and meta-analysis of randomized control trials. BMC sports science, medicine and rehabilitation. 2021;13(1):91.
- Tumilty S, Mani R, Baxter GD. Photobiomodulation and eccentric exercise for Achilles tendinopathy: a randomized controlled trial. Lasers Med Sci. 2016;31(1):127-135.
Do you feel like you want to know more, but don't know where to start? Join our course for Achilles Tendinopathy to learn how to take charge of your own health!
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.